I was honored and so excited to be interviewed by Photographer & Guest Writer, Marj Kleinman for her article at TocaBoca.com. She and I have much in common, including a deep passion for child life and play in hospitals, and the fact that we are both alums from Saint Ann’s School in Brooklyn, NY. She is a talented artist and used her creativity to write a photo journal of child life and play at Maimonides Hospital. I will publish that here next week. The Toca Boca article is reprinted here in full below.
Child life specialists support kids and families in a hospital environment, reducing stress and increasing joy.

- BY
- Marj Kleinman, Toca Magazine Guest Writer
When I tell someone that I volunteer in pediatric hospitals, I usually spot a sad face across from me. That response is understandable, given that hospitals can be scary and sometimes painful and upsetting. But in fact, there’s no greater place to see joy and resilience on display, all through kids’ natural passion for play.
Whether at their doctor’s office or in the ER, kids find a way to play, particularly with encouragement. Most children’s hospitals today come equipped with a playroom and a bevy of materials and activities, so kids can be kids while hospitalized. Once they see a playroom full of toys, messy finger paints and a silly guy blowing bubbles, they know this place is made for them and they will probably feel safe there. There’s even a team of people whose job is to play with your child: the child life specialists. They become parents’ partners in health and healing.
Meet the child life team: Your play partners
Many parents are surprised to learn that there’s a person solely focused on your child’s emotional health during a hospital stay — and they do it mainly through play. Child life specialists (CLSs) help kids and families adapt to the hospital environment and support them in understanding what’s taking place, thereby reducing the stress of a hospitalization. CLSs are trained in child development and play theory, as well anatomy, research methodology, sociocultural issues, ethics, family systems and bereavement, among other things. They also act as a bridge and advocate with your medical team. Child life departments often include art and music therapists, and are visited by yoga and mindfulness teachers, clowns and other practitioners.
Language of play
Play is the universal language of childhood — in fact, when CLSs assess their patients, they’re watching how kids communicate via play. I spoke to Deborah B. Vilas, a CLS and social worker who teaches child life graduate students at Bank Street College of Education. Vilas says, “Young children won’t sit down and say, ‘I felt sad today and I think I’m anxious about the medical treatment I’m getting.’ When children are playing, they act out scenarios and show us what they’re feeling; they show us what they understand, what they’re capable of and what their coping mechanisms are.” This may seem obvious, but in some hospitals, there’s a misconception that play is frivolous or low on the priority totem pole.
Young children won’t sit down and say, ‘I felt sad today and I think I’m anxious about the medical treatment I’m getting.’
Vilas reminds us, “It’s been proven that when children have play opportunities that they need less medicine, less anesthesia, are more compliant and get better faster. The benefits of play reach beyond the child to assist medical personnel and influence the hospital’s bottom line.”
Benefits of play
According to the American Academy of Pediatrics (AAP), “Play is essential to development because it contributes to the cognitive, physical, social, and emotional well-being of children and youth. Play also offers an ideal opportunity for parents to engage fully with their children.” Why would all that stop at the hospital? The AAP goes on to state that hospital play is a necessity that helps kids cope with treatment and stay on track, developmentally. The uses and benefits of play in medical settings are varied and significant.
At its essence, play provides a safe space for kids to experiment with unfamiliar and often scary experiences. Through open-ended play, kids can take in new information at their own pace, re-create situations and play out fears until they are familiar enough to gain a sense of mastery over the situation. When supported by an empathetic parent or CLS, this process is deepened and they can better process and release feelings.
At its essence, play provides a safe space for kids to experiment with unfamiliar and often scary experiences.
Open-ended and child-centered play, in particular, are highly beneficial, as they provide opportunities for kids to immerse themselves more deeply in play and lead from a sense of agency. Unfortunately, free play has been on the decline due to our hurried and jam-packed, overscheduled and tech-filled lifestyles, yet it is necessary for skill development, self-regulation, independent thinking and creative problem solving. In the hospital, where kids lack choices, it’s even more crucial to let kids be in charge.
Medical play
One of the roles of the CLS is to normalize the hospital experience through play. They might do familiarization activities, for example, building a robot using a bedpan, tongue depressors and IV tubing, all taped together with bandages. Suddenly medical supplies aren’t scary, cold, weird objects that only doctors and nurses use, and kids can “hack” the hospital.
Going a step further, medical play with a toy doctor’s kit and/or real medical supplies can 1.) educate children about an upcoming procedure, 2.) let them process their experience, before, during or after a procedure, and 3.) put the child back in the driver’s seat.

Children experience a strong sense of helplessness, vulnerability and anxiety when faced with uncertainty and misconceptions (let’s face it, so do grownups). Procedural support helps educate, greatly reducing feelings of unpredictability, and increases a level of mastery.
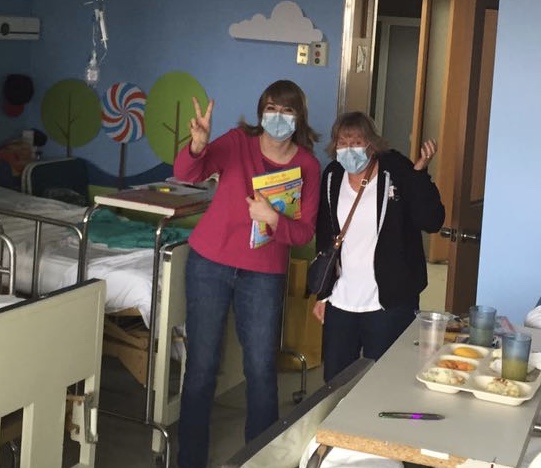
Meghan Amorosa, child life specialist at Brooklyn Hospital Center in Brooklyn, N.Y., says, “A really big part of medical play is about giving patients choice and control over their own hospital experience. Instead of being the patient, they become the doctor and play on their own little patient.” She observed that Jan (pictured above) gave the doll a lot of shots, which is typical in patients who’ve been poked a lot. In fact, “If a kid gives a doll a million shots, they’re showing you how painful that was for him,” says Vilas.
A really big part of medical play is about giving patients choice and control over their own hospital experience.

Movement also plays a key role in healing, which is why doctors want patients up and walking almost right after surgery. If kids can get out of bed and step on bubble wrap or a floor piano, ride a hospital wagon around the unit, or skate down the hallway on their IV pole, they get the blood circulating, feel more energized and also empowered at the same time.
Play is powerful and can be tailored towards your child’s individual age, temperament and tastes. Read on to find out 10 ways to support kids going to the hospital, as patients or visitors.
Marj Kleinman is a Brooklyn based photographer and children’s media producer with a master’s in educational psychology.