
Please welcome our guest blogger, Christina Connors, who I interviewed after she connected with me on Linked In and sent me samples of her incredible Get Well Maps.
What inspired you to create these maps? My son’s medical experience in 2014, and my desire to help other children and families facing medical challenges, inspired me to create Get Well Maps. Andrew was 5 years old when he was hospitalized with bilateral pneumonia and H1N1 flu, and his condition quickly became life threatening. He was air lifted to our closest pediatric hospital (~2 hours away) and was transferred to the PICU secondary to respiratory failure. I felt completely helpless to care for him. There were so many uncertainties. My “Mama Bear” impulses were raging, and yet my background as an Occupational Therapist was underpinning every effort I made to advocate for my child.

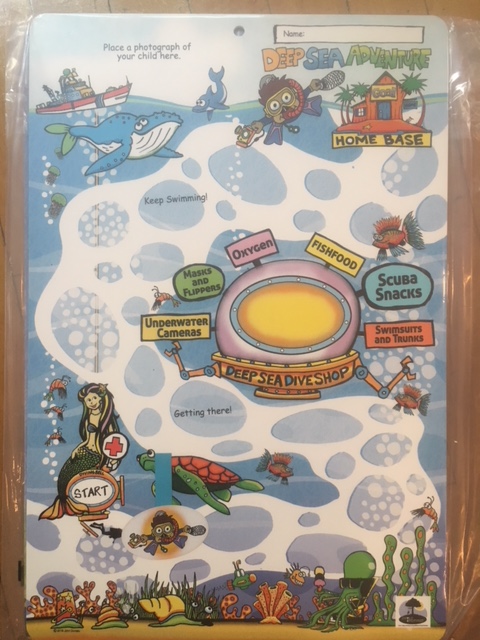
I felt compelled to have a visual that would depict his “Road Home”, because despite the uncertainty of prognosis, timeline or discharge plan, we needed to SEE our goal of getting home in the midst of adversity. I asked my childhood friend to make a map that had a road, photo of our home and matchbox car to move along as his condition progressed (My son has always loved anything with wheels☺). She was eager to do anything to help, but found it strange that my request of her was a “craft project” (Child Life Specialists & OTs get it☺). She graciously obliged, anyways. What began as a desperate mother’s attempt to provide a tool to help her child, began to draw interest from his medical team, and sparked communication that connected us throughout his care (“Is that your house?”, “Do you like to play outside?”, “Buddy, you’ve already rounded that bend”…). It was months after our experience, and after becoming involved in our pediatric hospital’s Family Advisory Committee, that another parent encouraged me to develop this idea in a way that would help other children and families throughout their medical experiences.

What was the process like from your idea to creating the product and your company? I would be lying if I said I wasn’t scared! I was exposing a time in our family’s life that held much vulnerability. But I was also excited about the possibility of having a creative outlet that helped me process our experience in a way that helped others. My faith was strengthened by our experience, and I felt like I was being called into this work. I felt that this was a unique opportunity to combine my experience as a parent and healthcare professional (& my husband is an educator) to make a positive impact in the healthcare experiences of other children and families. I began slowly. Brainstorming, then drafting prototypes, researching materials, production options, searching for the right illustrator, and learning the basics of establishing a business. I use the analogy of a foggy road when I think about the process of transforming an idea into a company, and even now as I continue to navigate and evolve. I can’t always see where I am headed because the road is foggy, but when I have faith enough to move forward, the fog lifts briefly and becomes a little clearer just in front of me, which in turn gives me the confidence to keep going. (Just can’t seem to get away from the road/car analogies!)
Can you tell us a bit about your work as an OT and your experience as a mom? I graduated from the Occupational Therapy program at Towson University in 2002, and have been practicing as an Occupational Therapist for 15 years. I became interested in Occupational Therapy after my Aunt was in a car accident and sustained a C4-C5 spinal cord injury. It was the 1st time my family was truly impacted by disability and I was inspired to learn more about the professionals that were helping her. Since beginning my career as an OT, I have always had an equal love of pediatric and adult rehabilitation. I have experience in hospital, inpatient rehabilitation, home healthcare and school settings. I have always found my work as an OT very rewarding, and am very passionate about working with individuals with neurological disorders and sensory needs. My greatest loves… my hubbie, Mike, and my 2 children are at the center of my world. There was a lot we experienced emotionally as a family during and following my son’s hospitalization that changed my perspective as a mom. I don’t worry as much about small decisions and details, don’t take as much for granted, and really value the importance of finding moments of “calm” in our hectic day-to-day routines. Their love, support, and boundless energy are driving forces behind Child Inspired.
What do you want parents and medical staff to know about children in hospitals? I think many already know, but I think ALL medical professionals need to know that (many, if not most) children and families are not processing auditory information effectively during stressful medical events. Children and families want (and need) medical teams to disclose accurate and honest medical information, but it needs to be delivered with a compassionate, child-centered approach. Don’t be scared of informing children and parents of setbacks or regressions in progress. They know setbacks occur. They just need consistent, jargon-free language that helps them understand what is happening and supports them through the disappointment. Families and medical professionals also need to know that emotional healing will often take much longer than physical healing, and need to be educated on resources that the family can access if emotional or behavioral concerns arise after discharge.
What are your hopes for your company? My hope for Child Inspired is that our Get Well Maps will become a model for child-centered discharge planning, and that our tools will also help children and families visualize their progress as they re-integrate back into school and community activities after medical events. In this fast-paced, digital age where much of what our children encounter is instant gratification, many children need support and encouragement as they work towards goals that require time and perseverance. It is my hope that our Maps facilitate positive, encouraging language and communication between children and the adults providing their care.
Do you have any tips for how parents and child life specialists might use these maps? I love your profession and the amazing work that you do with children, siblings and families, as well as the work you do to model and advocate for child-centered care among your other medical colleagues. I think that Child Life Specialists can play a pivotal role in daily medical rounding and discharge planning, and that Get Well Maps provide a method for facilitating child-centered communication and visually tracking medical progress. A Get Well Map is fun, and individualized to the child’s interests and goal, therefore, it reduces anxiety by helping you relay and reinforce information discussed in medical rounding (often laden with medical jargon) in a way that is developmentally appropriate and child-centered. Contact us to learn more about how a CCLS is using Get Well Maps with children after bone marrow transplants, and how her unit now has a physician order and pathway to initiate Child Life assessment and intervention (including Get Well Maps) from diagnosis to discharge.
Anything else you want us to know? Thank you for all that you do! As always, I would love to collaborate with you and your teams to develop solutions for your patient populations and healthcare organizations.























 Guest Blogger Heather Beal is a military veteran with 23 years of crisis management and operational planning experience that she draws upon daily in her battle to raise two well-prepared, happy, curious, and intelligent children. As a trained emergency manager and parent, she saw the need to provide age-appropriate disaster preparedness information to young children in a way that empowered rather than frightened them. She is currently writing additional books to cover a greater spectrum of potential disasters children may face.
Guest Blogger Heather Beal is a military veteran with 23 years of crisis management and operational planning experience that she draws upon daily in her battle to raise two well-prepared, happy, curious, and intelligent children. As a trained emergency manager and parent, she saw the need to provide age-appropriate disaster preparedness information to young children in a way that empowered rather than frightened them. She is currently writing additional books to cover a greater spectrum of potential disasters children may face.


 (photo by Jiri Kralovec)
(photo by Jiri Kralovec)
 (photo by Jiri Kralovec)
(photo by Jiri Kralovec) (photo by Jiri Kralovec)
(photo by Jiri Kralovec)
 (photo by Jiri Kralovec)
(photo by Jiri Kralovec) (photo by Jiri Kralovec)
(photo by Jiri Kralovec) (photo by Jiri Kralovec)
(photo by Jiri Kralovec) (photo by Jiri Kralovec)
(photo by Jiri Kralovec) (photo by Jiri Kralovec)
(photo by Jiri Kralovec)






























